
There is a very specific kind of question that tends to appear after a few years of living with PMDD.
Not at the beginning, when everything feels confusing and new. But later.
When you have enough cycles behind you to notice a pattern.
You start to realise that what once felt intense now feels overwhelming. That the emotional drop is sharper. That it takes longer to come back to yourself. That the “good” part of the month feels shorter than it used to…
And quietly, almost reluctantly, the question forms:
Is this actually getting worse with age?
It is a hard question to ask because it carries a lot underneath it. Fear, frustration, sometimes even grief for how things used to feel.
For many women, PMDD can intensify over time. But it does not do so in a straight, predictable line. And more importantly, it is not a fixed path.
What we see, both in research and in real life, is that symptoms tend to evolve. They are shaped by hormonal changes, yes, but also by stress, nervous system load, lifestyle, and how early support was introduced.
So instead of a simple yes or no, what matters more is understanding why it can feel worse and what actually changes as you move through different life stages.
PMDD affects around 3 to 8 percent of menstruating women globally¹. That number alone already tells us this is not rare, even if it is often misunderstood.
When researchers look at how PMDD changes over time, a few consistent patterns appear:
- Symptoms often increase in perceived severity with age, especially emotional symptoms²
- Women with PMDD show heightened sensitivity to hormonal fluctuations, rather than abnormal hormone levels³
- Mood-related symptoms such as irritability, anxiety, and depression tend to become more disruptive in daily life over time⁴
One important nuance here: it is not that hormones become “worse” as you age.
It is that your brain’s response to hormonal change can become more reactive, especially when other factors are layered on top.
Why PMDD can feel worse over time
In your teens and early twenties, hormones tend to follow a more predictable rhythm.
Estrogen rises, ovulation happens, progesterone increases, and then everything resets.
As you move into your thirties and especially closer to perimenopause (35 and up), that rhythm becomes less consistent.
- Estrogen can rise and fall more unpredictably
- Progesterone production may become weaker or inconsistent
- You may not ovulate every cycle
For a PMDD brain, which is already sensitive to change, this instability can feel like amplifying the signal.
The nervous system carries more load
PMDD is often described as a hormonal condition, but it is just as much about the nervous system.
Over time, life adds layers:
- Work pressure
- Relationship stress
- Sleep disruption
- Emotional fatigue
- More responsibilities overall
Research shows that women with PMDD experience heightened stress responses and altered cortisol patterns, particularly in the luteal phase⁵.
So when the nervous system is already stretched, the hormonal shift before your period can feel much harder to tolerate.
The impact of unsupported symptoms over time
There is another layer that often gets missed.
When PMDD symptoms are not recognised or supported, the body doesn’t just reset each month. It accumulates stress.
Over time, this can lead to a more dysregulated nervous system:
- Lower stress tolerance
- Slower recovery after each cycle
- A lingering sense of emotional fragility
For many women, this is also shaped by years of misdiagnosis or dismissal.
Repeated cycles of distress without support can build into something deeper, sometimes even mirroring patterns of chronic stress or complex trauma.
This helps explain why PMDD is linked to higher rates of suicidal ideation(17) and attempts.
Not just because of the hormones, but because of the accumulation of unsupported experiences over time.
Repetition strengthens the pattern
PMDD is cyclical, which means it repeats.
And repetition matters.
Over years of cycling through intense emotional states, the brain can become more efficient at entering anxiety or low mood, reinforcing negative thought loops or anticipating distress before it even begins.
This is one of the reasons tools like a symptom tracker become so important. They interrupt that automatic loop and create awareness.
Without that awareness, the cycle can feel like it is tightening over time.
The connection with the teenage years
If you look back, many women can trace early signs to their teenage years.
It may not have been labelled as PMDD at the time. Possibly it was labelled as PMS instead and it might have looked like:
- Strong mood swings
- Anxiety before periods
- Feeling emotionally overwhelmed in certain weeks
Research suggests PMDD is linked to genetic and neurological sensitivity to hormones, not just the hormones themselves⁶.
This means early symptoms are not random. They are often the beginning of a pattern.
And this is where early support becomes crucial.
When PMDD is recognised and supported earlier:
- The nervous system has more capacity to adapt
- Patterns are less deeply ingrained
- Symptoms are often easier to manage later
When it is missed or dismissed, it can gradually intensify over time, rooted in the confusion that it generates.
Perimenopause: the phase where symptoms often peak
If there is one stage where PMDD tends to feel most intense, it is perimenopause.
This phase can last anywhere from four to ten years before menopause, and it is defined by hormonal instability.
What changes here:
- Estrogen fluctuates more dramatically
- Progesterone steadily declines
- Sleep often becomes lighter and more fragmented
- Stress tolerance decreases
For women with a history of PMDD, studies show an increased risk of more severe mood symptoms during this transition⁷.
Common experiences during this phase include stronger irritability or rage, increased anxiety or panic, more persistent low mood or brain fog and reduced focus.
It is not just the hormones. It is the unpredictability of them.
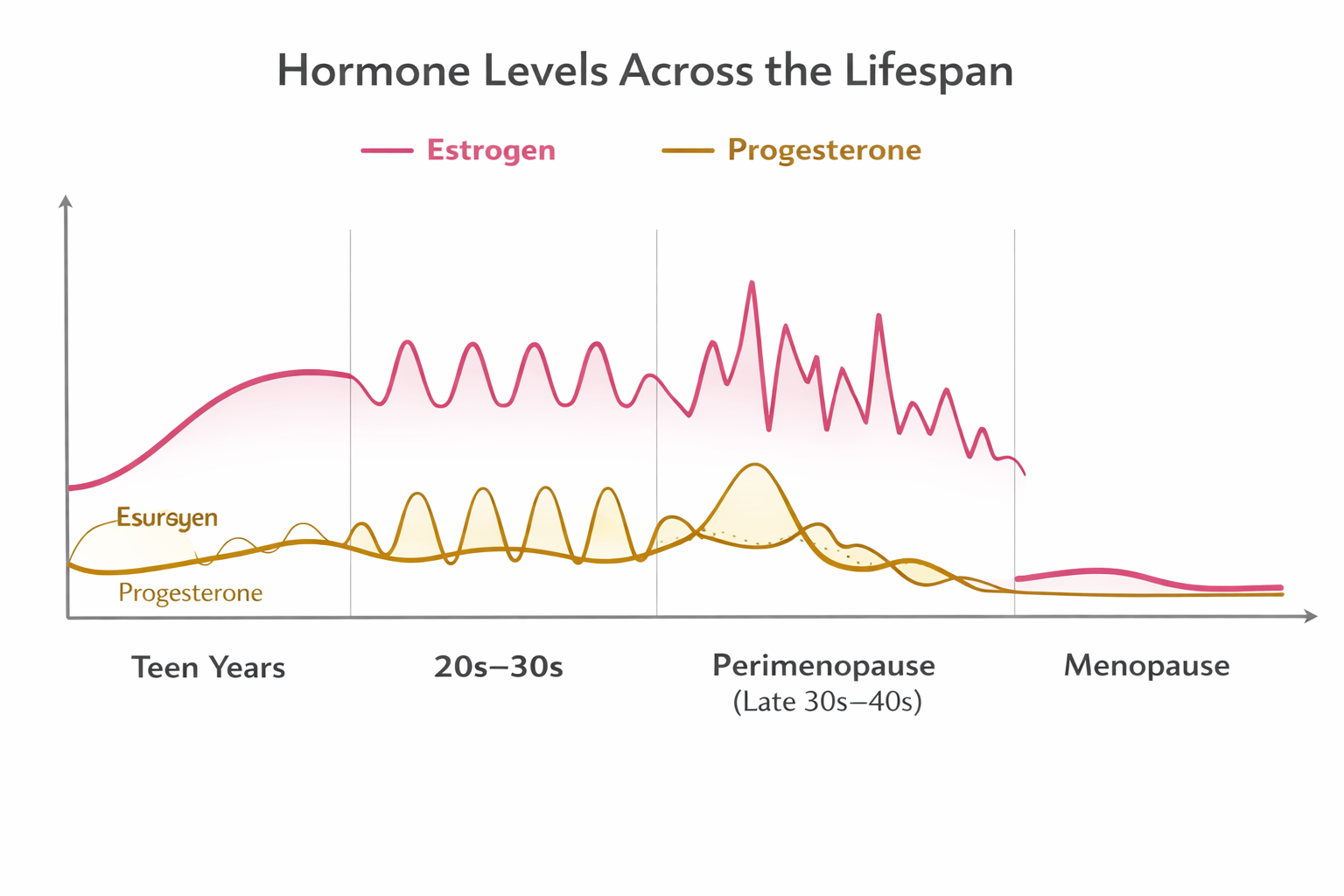
How hormones change over time
Here is a simplified way to understand what is happening across different life stages:
Hormonal patterns across the lifespan
Teen years¹²
- Estrogen: gradual rise and stabilisation
- Progesterone: begins cycling after ovulation starts
20s to 30s¹³
- Estrogen: consistent cyclical rise and fall
- Progesterone: stable post ovulation increase each cycle
Late 30s to 40s (Perimenopause)¹⁴
- Estrogen: irregular spikes and drops
- Progesterone: overall decline, less consistent ovulation
Menopause (1 year past your last period -average age 51)¹⁵
- Estrogen: low and stable
- Progesterone: very low and stable
The key point is this: PMDD is triggered by change. And perimenopause is a time of constant hormonal change.

The estrogen–dopamine connection
Estrogen doesn’t only affect your cycle. It also supports dopamine in the brain (18).
Dopamine plays a key role in focus, motivation, and emotional regulation.
When estrogen is more stable (like in your 20s), these systems tend to feel easier to manage.
But as estrogen begins to fluctuate or decline, dopamine support becomes less consistent.
This can show up as:
- More emotional sensitivity
- Difficulty focusing or making decisions
- Feeling more overwhelmed than before
For women with PMDD and ADHD traits, this shift can feel especially noticeable.
ADHD in women is often more mood-based than hyperactive, including emotional dysregulation, overwhelm, and low frustration tolerance.
These symptoms may have been manageable earlier in life, but hormonal changes can make them feel much harder to navigate.
For some, this is the first time things start to feel unmanageable.
And when combined with PMDD, it can amplify both mood and cognitive symptoms.
Does PMDD improve after menopause?
For many women, yes.
Once menopause is reached:
- Hormones stabilise at lower levels
- The cyclical trigger disappears
This often lead to a significant complete resolution of PMDD symptoms as PMDD is tied to the menstrual cycle⁸.
However, the transition into menopause and post-menopause can still come with symptoms and this is where support is most needed.
What actually makes symptoms worse over time
Hormones are only one part of the picture.
Research and clinical experience both point to several factors that can amplify PMDD symptoms:
- Chronic sleep disruption
- Blood sugar instability
- Nutrient deficiencies
- High and sustained stress
- Lack of movement or recovery
For example, low vitamin D levels have been linked to worsened mood symptoms in the premenstrual phase⁹.
Cognitive patterns also play a role.
Studies show increased negative thought loops during the luteal phase, which can intensify emotional symptoms¹⁰.
Over time, these factors can compound if they are not addressed.
Treatment: does it change with age?
Treatment does not become less effective with age, but it often needs to become more personalised.
Common approaches include:
- SSRIs
These remain one of the most researched treatments in the traditional medicine for PMDD, with studies showing up to 60 to 70 percent improvement in symptoms¹¹. They can be used daily or only during the luteal phase, depending on the individual. - Hormone Replacement Therapies
These aim to stabilise or suppress hormonal fluctuations, which can reduce symptoms for some women. - Integrative support
This is often where long term change happens:- Nutrition that supports blood sugar and hormones
- Nervous system regulation
- Consistent sleep patterns
- Strength and movement
- Targeted supplementation
The most effective approach is usually not one single intervention, but a combination.
So, does PMDD get worse with age?
For many women, symptoms do become more intense over time, especially as they approach perimenopause.
But that does not mean it is inevitable or irreversible.
What changes the trajectory is early awareness, consistent support and addressing both hormones and the nervous system.
A more grounded perspective
PMDD is not something you simply outgrow. But it is also not something that has to keep escalating.
When you start to understand your patterns, support your body properly, and work with your cycle instead of against it, things begin to shift.
Not overnight. But gradually.
Symptoms can become:
- More predictable
- Less intense
- Easier to recover from
If this resonates, a good place to start is with awareness. Tracking your cycle. Noticing patterns. Building from there… We have created the PMDD Rehab course for that purpose, to build the education and tools you need to understand your cycle.
And if you need a more individual approach, one-on-one support can help you work closely with your unique cycle pattern, symptoms, life stage and environment, so you’re not trying to figure it all out on your own.
REFERENCES
- Reilly TJ, Patel S, Unachukwu IC, et al. The prevalence of premenstrual dysphoric disorder: systematic review and meta-analysis. J Affect Disord. 2024;349:534–540.
- Hantsoo L, Epperson CN. Premenstrual dysphoric disorder: epidemiology and treatment. Curr Psychiatry Rep. 2015;17(11):87.
- Schmidt PJ, Nieman LK, Danaceau MA, et al. Differential behavioral effects of gonadal steroids in women with and without premenstrual syndrome. N Engl J Med. 1998;338(4):209–216.
- Rapkin AJ, Akopians AL. Pathophysiology of premenstrual syndrome and premenstrual dysphoric disorder. Menopause Int. 2012;18(2):52–59.
- Beddig T, Reinhard I, Kuehner C. Stress, mood, and cortisol during daily life in women with PMDD. Psychoneuroendocrinology. 2019;109:104372.
- Huo L, Straub RE, Roca C, et al. Risk for premenstrual dysphoric disorder is associated with genetic variation in ESR1. Biol Psychiatry. 2007;62(8):925–933.
- Gordon JL, Eisenlohr-Moul TA, Rubinow DR, et al. Estradiol variability and mood in the menopause transition. Clin Psychol Sci. 2016;4(5):919–935.
- Freeman EW. Premenstrual syndrome and premenstrual dysphoric disorder: definitions and diagnosis. Psychoneuroendocrinology. 2010;35(2):168–175.
- Abdi F, Ozgoli G, Rahnemaie FS. The role of vitamin D and calcium in premenstrual syndrome: a systematic review. Obstet Gynecol Sci. 2019;62(2):73–86.
- Beddig T, Reinhard I, Ebner-Priemer U, et al. Cognitive and affective states in women with PMDD: an EMA study. Behav Res Ther. 2020;131:103613.
- Shah NR, Jones JB, Aperi J, et al. SSRIs for premenstrual syndrome and PMDD: a meta-analysis. Obstet Gynecol. 2008;111(5):1175–1182.
- Apter D. Development of the hypothalamic-pituitary-ovarian axis. Ann N Y Acad Sci. 1997;816:9–21.
- Rapkin AJ, Akopians AL. Pathophysiology of premenstrual syndrome and PMDD. Menopause Int. 2012;18(2):52–59.
- Gordon JL, Eisenlohr-Moul TA, Rubinow DR, et al. Estradiol variability and mood during the menopause transition. Clin Psychol Sci. 2016;4(5):919–935.
- Prior JC. Perimenopause: the complex endocrinology of the menopausal transition. Endocr Rev. 1998;19(4):397–428.
- Burger HG, Hale GE, Robertson DM, Dennerstein L. Hormonal changes during the menopausal transition. Maturitas. 2007;57(3):295–305.
- Eisenlohr-Moul TA, et al. Premenstrual Dysphoric Disorder and Risk for Suicidal Thoughts and Behaviors: A Systematic Review. Journal of Clinical Psychiatry. 2017;78(9):e1234–e1242.
- Jacobs E, D'Esposito M. Estrogen shapes dopamine-dependent cognitive processes: implications for women's health. Journal of Neuroscience. 2011;31(14):5286–5293.
Remember: this post is for informational purposes only and may not be the best fit for you and your personal situation. It shall not be construed as medical advice. The information and education provided here is not intended or implied to supplement or replace professional medical treatment, advice, and/or diagnosis. Always check with your own physician or qualified medical professional before trying or implementing any information shared in this article.
Affiliate Disclosure
This blog post may contain affiliate links. This means we may receive a small commission if you choose to purchase through these links, at no additional cost to you. We only share products we personally use, trust, and recommend in our own work with clients.
